The Ultimate Clinical Guide to the Farnsworth D-15 Color Vision Test
The Farnsworth D-15 color vision test (also known as the Farnsworth-Munsell D-15) is a vital, albeit specialized, tool in the clinical assessment of color vision deficiency. While the ubiquitous Ishihara plates excel at rapid screening for red-green deficiencies, the D-15 goes a step further. It is a 15-disc hue arrangement test designed to assess both the severity and the specific type of color vision deficiency (protan, deutan, or tritan).
Crucially, the primary clinical and occupational value of the D-15 test lies in its ability to separate moderate to strong color vision defects from mild ones. For occupational screeners, HR safety officers, and optometrists, understanding the nuances of this test—from lighting standards to handling confusing results—is essential for accurate diagnosis and career counseling.
How to Administer the Farnsworth D15 Test

Proper administration of the D15 hue test procedure is paramount. Unlike digital tests or simple plate readings, the D-15 requires physical interaction and highly specific environmental controls.
Setup & Lighting Verification Standards
A critical error in many modern clinics is the assumption that any bright room light is sufficient for color vision testing. The standard medical requirement states the test must be performed under “MacBeth Daylight” (CIE Illuminant C or D65) or lighting that accurately simulates natural daylight.
The proliferation of modern commercial LED bulbs has complicated this. Standard office LEDs often have poor color rendering capabilities, particularly in the red spectrum, which can artificially induce errors or mask mild deficiencies.
How to verify your clinic’s lighting:
- Color Rendering Index (CRI): Ensure your lighting has a CRI of 90 or higher.
- Color Temperature: The light source should have a color temperature between 6000K and 7000K to properly mimic standard daylight.
- Positioning: Light should fall evenly on the testing surface at a 45-degree angle to minimize glare on the plastic caps.
Step-by-Step Patient Instructions
The way you explain the how to perform the farnsworth d15 procedure directly impacts the accuracy of the results. Patients must arrange the 15 colored caps in hue order, starting from a fixed reference cap.
Recommended Patient Script:“In front of you is a fixed reference cap. I want you to look at the remaining loose caps and find the one that most closely matches the color of this reference cap. Place it right next to it. Then, find the cap that most closely matches the one you just placed, and put it next in line. Continue this until all caps are arranged in a gradual color sequence. Take your time, but try to complete it within a couple of minutes.”
Farnsworth D15 Scoring and Interpretation
Once the patient completes the arrangement, the clinician must interpret the sequence. Farnsworth d15 scoring is done by flipping the caps over to reveal their numbered undersides and plotting this sequence on a specialized circular score sheet.
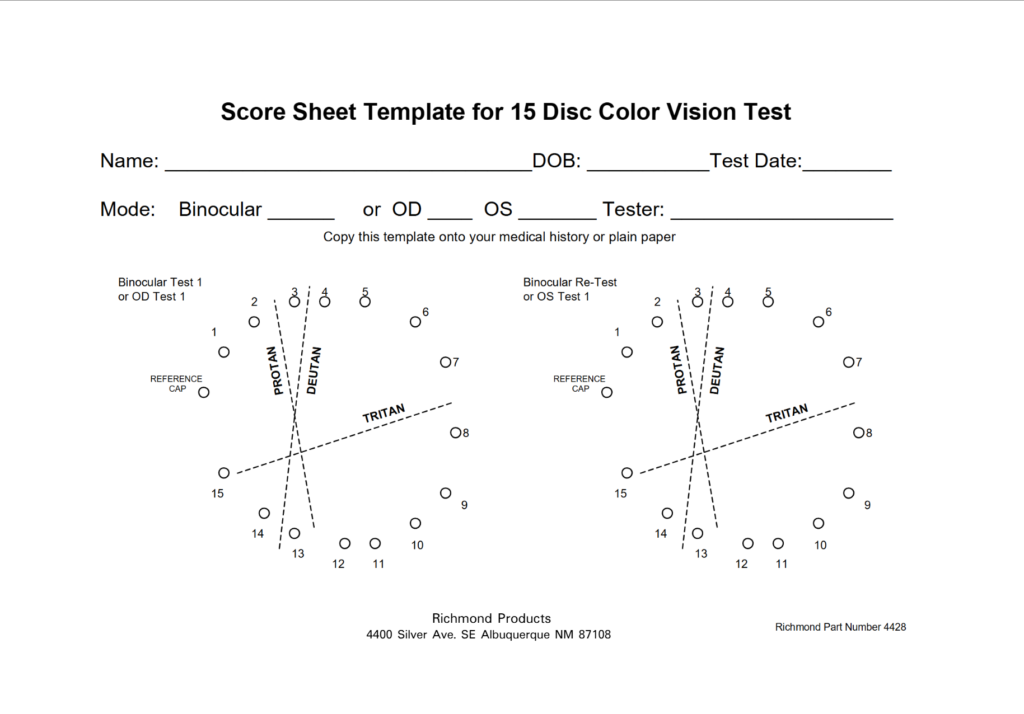
Plotting Results on the Scoring Sheet
To calculate the D15 color confusion index, connect the numbers on the score sheet in the exact order the patient arranged them.
- Normal Result: A normal result features a perfectly circular line where caps are in the correct 1-to-15 sequence, or it may feature only minor, adjacent swaps (e.g., 1-2-4-3-5). This is typically classed as normal or a very mild deficiency.
- Deficient Result: Deficiencies reveal themselves through “crossings”—lines that bisect the center of the scoring circle, connecting caps from opposite sides of the color wheel.
Identifying Protan, Deutan, and Tritan Axes
When crossings occur, the clinician must observe which direction the lines travel. The scoring sheet is pre-marked with confusion axes:
- Protan Axis: Crossings parallel to this axis indicate a red-blind deficiency.
- Deutan Axis: Crossings parallel to this axis indicate a green-blind deficiency.
- Tritan Axis: Crossings parallel to this axis indicate a blue-yellow deficiency (often associated with acquired ocular or systemic disease).
Handling “Anarchic” Results
Most textbooks perfectly illustrate clean Protan, Deutan, or Tritan error patterns. However, clinicians frequently encounter “anarchic” arrangements—random, scattered cap placements with multiple crossings that do not align with any known confusion axis.
What causes anarchic results?
- Acquired Color Vision Defects: Diseases affecting the macula or optic nerve (like optic neuritis or severe macular degeneration) often produce chaotic color perception rather than clean congenital axes.
- Cognitive Misunderstanding: The patient may not have understood the instructions and is simply placing caps randomly.
- Malingering: The patient may be intentionally failing the test, though this is difficult to prove without an anomaloscope.
Next Steps: If an anarchic result occurs, re-explain the instructions clearly and re-administer the test. If the result remains chaotic, suspect an acquired defect and proceed with a full ocular health workup.
Pass/Fail Criteria & Occupational Standards
The Farnsworth D-15 is heavily utilized in occupational health. It was specifically designed under the premise that individuals who can pass the test—even if they have a mild deficiency—can safely recognize critical surface color codes in the real world, such as electrical wiring, maps, or suspect clothing.
However, a major point of confusion for both patients and newer practitioners is how a “pass” is actually defined.
The Myth of a Universally Standardized “Pass”
There is no single, universally agreed-upon threshold for passing the Farnsworth D-15. Instead of a simple pass/fail grade, the score sheet reveals a spectrum of errors. It is up to the specific hiring agency to determine their risk tolerance.
When grading, examiners look at two types of errors:
- Adjacent Transpositions: Minor errors where a patient swaps two neighboring caps (e.g., placing cap 5 before cap 4). This is universally considered a normal/passing result.
- Major Crossings: Severe errors where a patient confuses caps from opposite sides of the color wheel (a cap difference of greater than 3).
Different agencies apply completely different thresholds regarding how many major crossings are allowed:
Industry-Specific Color Vision Standards
1. Law Enforcement & First Responders (The “Second Chance” Test) For most local and state police departments in the US and Canada, the D-15 acts as a highly valuable secondary test. Candidates are initially screened using the Ishihara dot test. Because the Ishihara is so strict, many capable candidates fail. If they fail, they are offered the D-15. In law enforcement, passing the D-15 (usually defined as having zero or only one major crossing) acts as a waiver, proving the candidate has enough functional color vision to identify vehicle colors or clothing descriptions in the field.
2. Aviation & The FAA (Crucial 2025 Update) Historically, the D-15 was an accepted alternative test for civilian pilots who failed their initial screening. However, regulations change rapidly. As of January 2025, the Federal Aviation Administration (FAA) no longer recognizes the Farnsworth D-15 as an acceptable color vision test for pilots. Pilots must now rely on modernized, FAA-approved digital alternatives like the CAD (Colour Assessment & Diagnosis) test or the Waggoner CCVT.
3. Military Standards Military branches often have strict, codified rules for the D-15 depending on the specific occupational specialty (MOS). For example, standard guidelines for the Canadian Military strictly define a pass as having no errors or only minor adjacent errors, allowing for a maximum of one (1) major crossing error. Two or more major crossings constitute a definitive failure, which restricts the recruit from specific combat, aviation, or electrical engineering roles.
Because of these varying standards, research notes the D-15 should not be the only test used for definitive job selection. Always consult the specific medical guidelines of the organization (e.g., FAA, local police, maritime agencies) you are screening for.
Patient Counseling: Explaining a “Mild” Deficiency
A frequent and challenging clinical scenario arises when a patient fails the Ishihara plates but passes the D-15. These patients have a mild deficiency. However, because they “see fine” in their daily lives, they often stubbornly believe their vision is perfectly normal.
How to counsel these patients:
- Validate their experience: Acknowledge that in 95% of daily tasks (driving, picking out clothes, watching TV), their color vision is completely functional.
- Explain the nuance: Use an analogy. Explain that their color vision is like a radio that is slightly out of tune. They can still hear the music perfectly well, but they might miss the subtle background notes. The Ishihara test looks for the background notes; the D-15 looks to see if they can hear the main melody.
- Discuss Occupational Impact: Be candid about color vision standards. Explain that while they passed the D-15, their failure on the Ishihara still classifies them as color deficient. Depending on the exact wording of a career’s medical requirements (e.g., “Must pass Ishihara”), this mild defect could still impact rigorous career prospects in aviation, military, or electrical fields.
How to Pass the Farnsworth D-15 Color Vision Test
If you are pursuing a career in law enforcement and recently failed the Ishihara dot test, the Farnsworth D-15 is often your lifeline. Many police departments, federal agencies, and public safety commissions offer the D-15 as an alternative screening or waiver test. Passing the D-15 demonstrates that your color vision deficiency is mild enough to safely perform your duties on patrol. Here are the most effective strategies to ensure you pass with confidence.
1. Understand What a “Passing Score” Looks Like
Unlike the Ishihara test, which demands perfect color perception, the D-15 test is forgiving of minor errors. The objective is to arrange 15 colored caps in a sequential hue gradient. To pass, you must avoid “major crossings.” A major crossing occurs if you sequence two caps that are on opposite sides of the color wheel. Minor transpositions—such as mixing up two caps that are right next to each other in the sequence—are generally considered passing by medical review boards.
2. Ensure Proper Clinical Lighting
Lighting drastically alters how your eyes perceive subtle hues. The clinical standard for administering the D-15 requires daylight-simulating illumination. If the testing room is illuminated by standard, warm-toned office tungsten or yellow fluorescent lights, a red-green deficiency will be artificially worsened. Politely advocate for yourself: ask the examiner to ensure the test is conducted under standardized lighting or near a window providing natural daylight.
3. Manage “Color Fatigue”
The Farnsworth D-15 is typically not a timed race. Staring intensely at the pastel caps for extended periods can cause color fatigue, a phenomenon where your photoreceptors become desensitized and the hues begin to bleed together. If you feel stuck, look away at a neutral white or gray wall for 10 to 15 seconds. This “resets” your vision, allowing you to return to the tray with fresh eyes.
How the D15 Compares to Other Color Vision Tests
To fully grasp the utility of the Farnsworth D-15, practitioners must understand where it fits within the broader clinical workflow. While top-ranking resources simply list different tests, understanding when and why to transition from one test to another is critical for accurate patient assessment.
The Clinical Workflow: When to Use the D15 Instead of Ishihara
The Ishihara pseudo-isochromatic plate test is a highly sensitive screener; if a patient has even a slight red-green defect, they will almost certainly fail. However, it cannot reliably categorize the severity of the defect or detect tritan (blue-yellow) deficiencies.
The D-15 should be used after an Ishihara failure to gather more detailed classification information. It is expressly designed to separate subjects into one of two groups: those with normal or mild color deficiency versus those with medium or strong color deficiency.
Farnsworth D15 vs. Lanthony Desaturated D-15
While both tests share the exact same administration procedure and score sheet template, their clinical applications differ vastly based on cap color saturation.
- Farnsworth D-15: Uses vivid, highly saturated colored discs. It is fairly easy for those with mild defects to pass, making a non-perfect score indicative of a strong color deficiency.
- Lanthony D-15: Uses artificially faded (desaturated) colored discs, making the arrangement task significantly more difficult. A non-perfect score indicates a mild color deficiency, making this test highly appropriate for detecting subtle acquired color defects. Crucially, the Lanthony test is not appropriate for patients who have already failed the standard Farnsworth D-15.
D-15 vs. Farnsworth-Munsell 100-Hue Test
The Farnsworth-Munsell 100-Hue test is the D-15’s larger sibling. While the 100-Hue provides a highly detailed, in-depth study of a patient’s color vision, it is incredibly time-consuming to administer and score. The D-15 was created as a direct modification of the 100-Hue specifically for faster classification in busy clinical and occupational settings.
D-15 vs. The Anomaloscope
The Nagel anomaloscope is widely considered the “gold standard” reference test for identifying and classifying red-green color deficiency. It requires the patient to make an exact color and luminance match using a specialized optical instrument.
- The Clinical Reality: While the anomaloscope is highly precise, the instruments are expensive, require significant training, and are rarely found outside of specialized research or occupational clinics.
- The Comparison: In contrast to the anomaloscope’s exact matching requirement, all of the D-15 hues are presented at the same time, allowing patients to use careful observation and even chance to arrange them into a natural color order. Consequently, the D-15 is an imperfect predictor compared to the anomaloscope, particularly for protanomalous (red-weak) trichromats who may use luminance cues to pass the D-15 despite having a significant deficit on the anomaloscope.
Quick Reference: Color Vision Test Comparison
| Test | Primary Purpose | Difficulty / Saturation | Time to Administer | Clinical Role |
| Ishihara Plates | Red-Green Screening | Low / High Saturation | < 1 minute | Baseline screener; high sensitivity for red-green defects. |
| Farnsworth D-15 | Classification (Severity & Type) | Moderate / High Saturation | 2–3 minutes | Determines if a defect is mild vs. moderate/severe. |
| Lanthony D-15 | Detecting Mild/Acquired Defects | High / Desaturated (Faded) | 3–5 minutes | Identifies mild defects in patients who pass the Farnsworth D-15. |
| FM 100-Hue | In-Depth Analysis | High / High Saturation | 15–20+ minutes | Granular analysis of color discrimination capabilities. |
| Anomaloscope | Gold Standard Diagnosis | Exact Matching | 10–15 minutes | The ultimate reference test for precise classification. |
Can You Take the Farnsworth D15 Test Online?
With the rise of telemedicine, many patients search for a d15 color blind test online or a free farnsworth d15 app.
Can you take it online? Yes, there are online versions available. However, consumers and clinicians must understand a massive caveat: online results are not equivalent to standardized clinical testing.
The accuracy of an online hue arrangement test depends entirely on the hardware being used. Screen brightness, monitor color calibration, TrueTone or blue-light-blocking software, and ambient room lighting will heavily skew the results. While an online test can be a fun self-screening tool to identify a gross, severe defect, it cannot be used for official medical or occupational clearance.
Why the Farnsworth D-15 is Easier with Colorblind Contacts
Before taking the Farnsworth D-15, it is crucial to clarify your testing conditions. While strict government, aviation, or military medicals often require uncorrected natural vision, many private sector employers, trade schools, and functional capacity evaluations allow the use of optical aids.
If your specific screening permits functional color correction—meaning they only care that you can accurately perform the job—colorblind contacts can significantly improve your performance.
Here is the optical science behind why they provide a distinct advantage:
- Targeted Spectral Filtering: Advanced lenses use notch-filtering technology to block the overlapping light waves responsible for red-green color confusion. This forcefully separates identical-looking hues, creating a sharp contrast between the D-15 color caps.
- Essential Visual Cues: While lenses cannot cure colorblindness, they distinctly shift the luminance (brightness) and saturation of specific colors. This provides your brain with secondary visual cues to correctly sequence the gradient and avoid the severe cross-spectrum errors that lead to a failing score.
- Bridging the Pass/Fail Gap: The D-15 test clinically permits minor cap reversals. For individuals with mild to moderate anomalous trichromacy, this enhanced contrast provides the exact optical boost needed to cross the passing threshold for strict occupational screenings.
Ready to improve your color contrast and tackle your vision screening with confidence?
👉 Get Your Colorkinds Colorblind Contact Lenses Today
Farnsworth D-15 Color Vision Test FAQ
The ultimate resource for clinical administration and occupational requirements.
Basic Understanding & Procedure
What is the Farnsworth D15 test?
It is a short 15-disc hue arrangement test used to assess color vision deficiency.
What does the D15 color vision test measure?
It measures the severity and type of color vision deficiency (protan, deutan, tritan) and a person’s ability to discriminate along key axes.
How is the Farnsworth D15 test performed?
A patient is asked to arrange 15 colored caps in hue order, starting from a fixed reference cap, under standard lighting.
Do I need special lighting for the Farnsworth D15 test?
Yes, it is highly recommended to use a light booth or lighting that simulates natural daylight (CIE Illuminant C or D65) to ensure accurate results.
Interpretation & Accuracy
How do you interpret Farnsworth D15 results?
Results are interpreted using a score sheet where the clinician connects the cap order to look for crossings; few or no crossings equal a normal or mild defect, while severe crossings align with specific confusion axes.
What is a normal result on the D15 test?
A normal result means all caps are arranged in the correct sequence or feature only minor adjacent swaps. This is typically classed as normal vision or a very mild deficiency.
How accurate is the Farnsworth D15 test?
The test has high specificity but reported sensitivities around 50–80%, meaning it is less sensitive than an anomaloscope and may miss mild defects.
Comparisons to Other Tests
When should you use the D15 instead of the Ishihara test?
The D-15 should be used after a patient fails the Ishihara test to gain more detailed information about the severity and type of the deficiency; it is also highly useful for monitoring acquired defects.
What is the difference between Farnsworth D15 and Lanthony D15?
The Farnsworth D-15 uses more saturated caps to split normal/mild from moderate/strong defects, whereas the Lanthony desaturated test uses fainter colors, making it harder and better suited to pick up milder defects.
How does the D15 test compare to the Farnsworth‑Munsell 100‑Hue test?
The D-15 is a shorter classification tool, while the 100-Hue is a more detailed but time-consuming test for in-depth color vision analysis.
Occupational & Law Enforcement Use
Why is the Farnsworth D15 test used for jobs?
It is heavily used in occupational counseling because it is designed so that those who pass can successfully recognize surface color codes, such as electrical wiring or suspect clothing descriptions in the field.
Is the D15 color vision test enough for occupational screening?
While often helpful, it is imperfect; research notes that it should not be the only test relied upon for definitive job selection.
What counts as a passing score on the D-15 for police officers?
Passing generally requires zero “major crossings” (diametrical crossings). This means your sequence does not connect caps from opposite sides of the color wheel. Minor transpositions (swapping two adjacent caps) are usually graded as a pass.
Can I wear colorblind contacts during the law enforcement medical exam?
No. Almost all law enforcement agencies strictly prohibit the use of color-correcting lenses (like Colorkinds or EnChroma) during the vision screening. Doctors are trained to check for the distinct red tint of these lenses. However, they are often permitted for daily use on patrol once you are sworn in.
If I fail the D-15, can I get a medical waiver?
It depends on the agency. Some municipal departments will allow an appeal where you can take a “field test” (identifying car colors or clothing at a distance), but many state and federal agencies may issue a hard disqualification if you fail the secondary D-15 test.
Does the FBI accept the D-15 color vision test?
Yes. The FBI allows applicants who fail the initial Ishihara screening to continue processing if they can successfully complete the Farnsworth D-15 color vision test.